The two most widely performed MTF vaginoplasty techniques produce a neovagina from very different tissue sources, with meaningfully different outcomes for depth, lubrication, recovery, and long-term care. Choosing between sigmoid colon vaginoplasty and penile inversion vaginoplasty is one of the most important decisions in your surgical planning, and no single answer fits every patient. Both pathways are available through the sex reassignment surgery programme at Phyathai 2 Hospital in Bangkok.
This article gives you an honest, side-by-side account of how each technique works, what it delivers, who it suits, and where the trade-offs lie.
Understanding the Two Main SRS Techniques
At their core, both penile inversion and sigmoid colon vaginoplasty share the same goal: creating a functional vulva and vaginal canal. What separates them is the tissue used to form the vaginal lining, and the consequences that flow from that single difference.
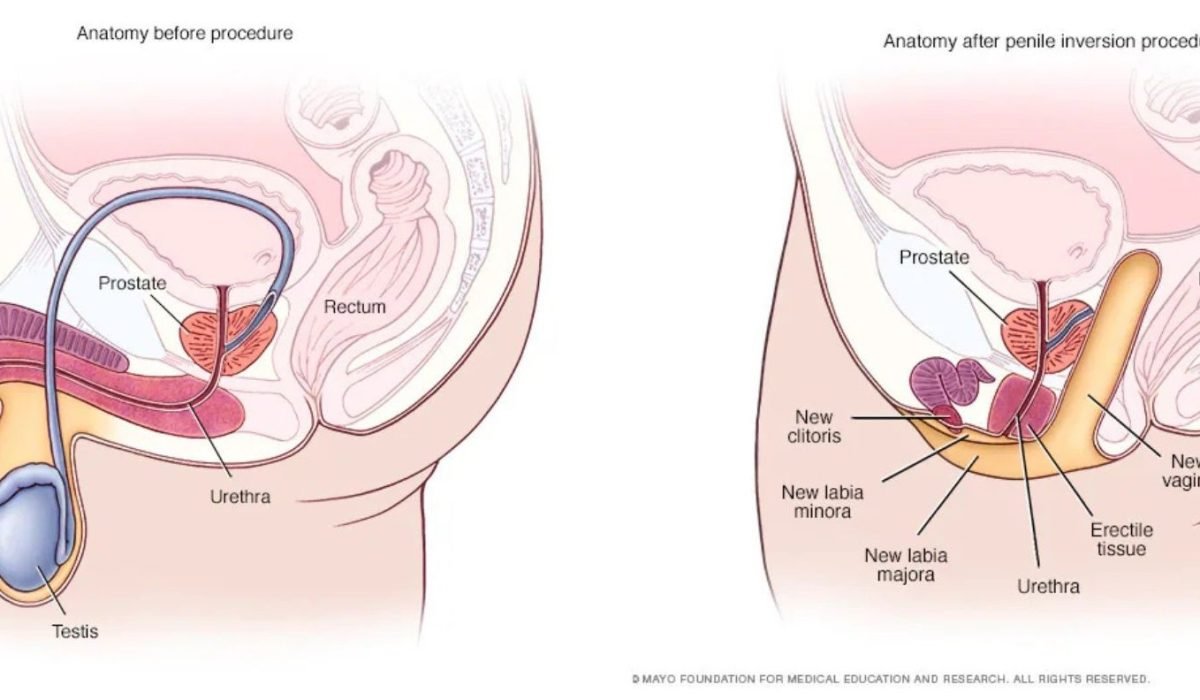
Penile inversion vaginoplasty uses existing genital skin, primarily from the penile shaft, with scrotal skin used where additional depth is needed. The penile skin is turned inside out to line a surgically created canal. It has been the dominant technique for over four decades and is chosen in around 80% of cases worldwide. If you want a full breakdown of how penile inversion works step by step, our detailed explainer on penile inversion vaginoplasty covers the complete picture.
Sigmoid colon vaginoplasty takes a 15 to 20 cm segment of the sigmoid colon, preserves its blood supply through the mesentery, and routes it through the pelvis to form the vaginal canal lining. The intestinal mucosa produces natural moisture. The outer genitalia — clitoris, labia, and urethral position — are constructed the same way as in penile inversion, using available penile and scrotal skin.
How Sigmoid Colon Vaginoplasty Works
The sigmoid colon is the S-shaped final section of the large intestine, positioned just before the rectum. Unlike skin, it is lined with a mucosa that naturally produces moisture. That property is what makes it useful for vaginal reconstruction.
Surgery typically involves a laparoscopic abdominal component, performed by a colorectal or abdominal surgeon working alongside the plastic and reconstructive surgeon. The process unfolds as follows:
- Bowel preparation.
One to two days before surgery, a liquid diet and laxative cleanse clear the sigmoid colon to reduce infection risk during resection. - Oestrogen stopped.
In line with WPATH guidelines, feminising hormones are discontinued two to four weeks before surgery to reduce clotting risk. - Pre-operative colonoscopy.
Standard practice for patients over 40, or those with any bowel history, to confirm the sigmoid colon is healthy and suitable for harvest. - Abdominal access.
Small laparoscopic incisions allow the surgeon to identify and mobilise a sigmoid colon segment with its vascular pedicle intact. - Resection and reanastomosis.
The selected segment is removed. The remaining bowel is rejoined above the resection site to restore continuity and normal digestive function. - Canal creation and positioning.
A perineal space is developed between the rectum and urethra. The sigmoid segment is brought through the pelvic cavity and sutured to the perineal skin at the vaginal opening. - Genital reconstruction.
Orchiectomy, clitoroplasty, labiaplasty, and urethroplasty proceed as in penile inversion, using the penile and scrotal skin for the external structures. - Closure.
Vaginal packing is placed, and abdominal incisions are closed.
One practical note on hair removal: because sigmoid colon tissue does not contain hair follicles, there is no pre-operative scrotal hair removal requirement. This is a meaningful difference for patients who have not yet begun or completed a hair removal course.

The Core Differences: A Head-to-Head Comparison
“The choice between techniques is not about which method is superior. It is about which outcome profile matches your anatomy, priorities, and long-term expectations.” Based on WPATH Standards of Care, Version 8, clinical guidance
The comparison below sets out the key differences across every factor that most patients are weighing:
| Feature | Penile Inversion (PIV) | Sigmoid Colon (SCV) |
|---|---|---|
| Tissue source | Penile and scrotal skin | Sigmoid colon segment (15-20 cm) |
| Typical depth | 12 to 16 cm | 14 to 19 cm |
| Self-lubrication | No — external lubricant required | Yes — from intestinal mucosa |
| Hair removal pre-surgery | Required (scrotal area, 6-12 months) | Not required |
| Surgery time | 4 to 6 hours | 5 to 7 hours |
| Hospital stay | 5 to 7 days | 7 to 10 days |
| Surgical complexity | Single-site; plastic surgeon only | Two-site: colorectal plus plastic surgeon |
| Bowel preparation | Not required | Required (1 to 2 days before surgery) |
| Long-term dilation | Lifelong; intensive first year | Less intensive; some ongoing maintenance |
| Primary complication risk | Vaginal stenosis (~5.7%) | Bowel-related complications (rare; more serious) |
| Medidash package price | From A$15,050 | From A$21,500 |
A 2025 retrospective study of 119 patients published in the Journal of Plastic, Reconstructive and Aesthetic Surgery found that sigmoid colon vaginoplasty provides self-lubricating mucosa, requires less dilation, enables a longer neovaginal canal, and may reduce the risks of stenosis and reoperation compared to penile inversion. The trade-off is greater surgical complexity and a longer initial recovery.
Who Is a Good Candidate for Each Technique?
Both techniques require the same WPATH SOC8 prerequisites: documented gender dysphoria, at least 12 consecutive months of feminising hormone therapy, age 18 or over, and appropriate mental health documentation. Beyond those shared requirements, anatomy and personal priorities shape the choice.
Penile inversion is typically recommended when:
- There is adequate penile and scrotal tissue to achieve the desired canal depth
- This is a first SRS procedure, and a simpler surgical approach is the preference
- Shorter in-hospital recovery is a priority
- The patient is willing to commit to the lifelong dilation schedule
- Budget is a consideration
Sigmoid colon vaginoplasty is typically recommended when:
- Penile length is limited, generally an erect measurement of less than approximately 5 cm, and adequate canal depth cannot reliably be achieved with skin inversion alone
- The patient strongly prioritises natural self-lubrication and a less intensive long-term dilation commitment
- This is revision surgery after a previous vaginoplasty, particularly where vaginal stenosis has developed following penile inversion
- Greater vaginal depth is a clear priority
Sigmoid colon vaginoplasty is not suitable when:
- There is a history of inflammatory bowel disease — Crohn’s disease or ulcerative colitis
- Previous major abdominal surgery has compromised access to the sigmoid colon
- Active bowel pathology has been identified at pre-operative colonoscopy
In a 2025 JPRAS series of 119 sigmoid colon vaginoplasty cases, 55.5% were primary procedures. The technique is not reserved exclusively for revision cases; it is appropriate as a first surgery when anatomy and priorities indicate it.

Recovery: The Key Differences Between the Two Pathways
The first weeks after surgery follow a broadly similar structure for both techniques. The meaningful difference is that sigmoid colon vaginoplasty involves recovery from two surgical sites rather than one, which extends the in-hospital phase and the return-to-activity timeline.
| Period | Penile Inversion | Sigmoid Colon |
|---|---|---|
| In hospital | 5 to 7 days | 7 to 10 days |
| Diet | Normal post-discharge | Liquid to soft food; bowel function monitored |
| Catheter | 10 to 14 days | 10 to 14 days |
| Dilation begins | Around day 5 | Around day 7 to 10 |
| Return to light activity | 4 to 6 weeks | 6 to 8 weeks |
| Penetrative intercourse | Approximately 3 months | Approximately 3 to 6 months |
| Long-term dilation | Multiple sessions daily; tapers over 12 months | Less intensive; introital maintenance ongoing |
A prospective study covering 30 primary sigmoid vaginoplasty procedures between 2023 and 2025, published in PMC, recorded a mean hospital stay of 8 days and a mean intraoperative neovaginal depth of 16 cm. Long-term follow-up confirmed patient satisfaction with both sexual function and depth.
Discharge management: Sigmoid colon tissue continues producing mucus for several months after surgery. Many patients find the volume noticeable in the first few months and manage this with a thin liner. For most, this reduces significantly as the tissue settles. It is a real consideration to discuss honestly with your surgeon before choosing this pathway.
For week-by-week detail on what recovery from vaginoplasty actually involves — dilation schedules, wound care, when you can fly home from Bangkok — the vaginoplasty recovery week-by-week guide walks through it in full.
A Third Option Worth Knowing: Peritoneal Pull-Through
Peritoneal pull-through vaginoplasty — often abbreviated to PPV — is a third technique that sits between penile inversion and sigmoid colon in terms of surgical complexity. It uses the peritoneum, a thin membrane that lines the abdominal cavity, to form the upper portion of the vaginal canal. The lower portion is constructed from penile skin, as in standard penile inversion.
PPV is performed laparoscopically and avoids the bowel resection required for sigmoid colon vaginoplasty. Natural moisture is produced by the peritoneal lining. It is increasingly used in revision cases and in patients with limited genital tissue who want to avoid an intestinal procedure. It also has the practical advantage of not requiring pre-operative hair removal, since the peritoneal tissue is hairless.
The key limitation is that long-term outcome data for PPV in transgender women are less established than for either penile inversion or sigmoid colon. It is not currently part of the Medidash package at Phyathai 2. Patients who want to understand whether PPV might apply to their situation are encouraged to raise it during their consultation.
How Medidash Supports This Decision at Phyathai 2
Phyathai 2 Hospital is a 550-bed, JCI-accredited institution in central Bangkok, with 27 specialist medical centres and a full on-site ICU. Surgery is performed by a lead surgeon who holds the position of Associate Professor of Plastic and Reconstructive Surgery at King Chulalongkorn Memorial Hospital, the institution where Thailand’s first SRS procedure took place in 1983.
For sigmoid colon vaginoplasty, an abdominal or colorectal surgeon joins the team for the bowel resection and reanastomosis component. Having this multidisciplinary capacity within a full-service hospital — rather than a specialty-only clinic — means that any bowel-related complication can be managed by the relevant specialist within the same institution.
The Medidash full-care pathway covers both techniques. The Penile Inversion Pathway starts from A$15,050; the Sigmoid Colon Pathway from A$21,500. Both include WPATH documentation review, surgical booking, hotel partner coordination, and 12 months of Australian-side aftercare with check-in calls at weeks 1, 4, 12, 26, and 52. Surgery is typically scheduled within four to eight weeks of approval. Full package details and the consultation request are on the sex reassignment surgery in Bangkok page.
For a full overview of the surgical landscape, documentation requirements, and what to prepare before travelling, the complete guide to SRS surgery in Thailand covers the broader picture.
Ready to Work Out Which Technique Is Right for You?
Understanding the differences is the right starting point. The next step is a conversation with a team that has clinical experience of both pathways, so the recommendation you receive reflects your anatomy and your goals rather than a generic preference.
Request a confidential consultation with Medidash. No commitment to proceed. Enquiries are answered within one business day, and your conversation is completely private. Contact Medidash to start your conversation.

Common Questions When Deciding Between Techniques
Is sigmoid colon vaginoplasty more dangerous than penile inversion?
Both techniques carry risk, but of different types. Penile inversion carries a higher rate of vaginal stenosis, at around 5.7% of cases. Sigmoid colon vaginoplasty carries a small but more serious risk of bowel-related complications, including anastomotic leak or bowel injury requiring reoperation. These major complications are rare: the 2025 PMC study of 30 primary sigmoid cases reported two major complications requiring reoperation, with no mortality. The important point is that a full-service hospital with on-site abdominal surgical teams and ICU — as Phyathai 2 provides — is the appropriate setting for sigmoid vaginoplasty, precisely because the backup infrastructure exists if it is needed.
Will I still need to dilate after sigmoid colon vaginoplasty?
Yes, though less intensively over the long term. Sigmoid colon tissue is more resistant to shrinkage than skin-based tissue, so the ongoing dilation schedule is less demanding. Dilation remains important at the introitus, where colon meets perineal skin, to prevent narrowing at that junction. The surgical team will give you a dilation protocol based on your anatomy and progress.
Does the mucus discharge from sigmoid vaginoplasty cause problems?
In the early months, it can be noticeable. The sigmoid lining continues to produce mucus, and some patients find the volume higher than they expected initially. Most patients see this reduce significantly within six to twelve months as the tissue adapts. For others, it remains manageable with a thin liner. This is a genuine trade-off of the technique that is worth discussing before making a decision, not something to minimise.
Can sigmoid colon vaginoplasty be my first surgery rather than a revision?
Yes. While the technique is commonly used after failed penile inversion, it is entirely appropriate as a primary procedure when limited tissue or depth requirements indicate it. In the 2025 JPRAS retrospective series of 119 cases, 55.5% were primary sigmoid colon vaginoplasty procedures.
How is the choice between techniques made during consultation?
Anatomy determines what is physically possible; your priorities determine what is right for you. The surgeon at Phyathai 2 will assess your available tissue, review your documentation, and give you a clear recommendation based on both. No patient is directed toward the more complex option unless it is genuinely indicated. Medidash coordinates this assessment as part of the initial consultation, which is free and carries no commitment.